
|
|
|
Clin. Cardiol. 23, 53–54 (2000)
Jong-Won Ha, M.D., Ph.D., Moon-Hyoung Lee, M.D., Byung-Chul Chang, M.D., Ph.D.,* Namsik Chung, M.D., Ph.D., June Kwan, M.D., Sang-Ho Cho, M.D., Ph.D.
Divisions of Cardiology and *Cardiovascular Surgery, Cardiovascular Center, Department of Pathology, Yonsei University College of Medicine, Seoul, Korea
A 40-year-old male patient presented with shortness of breath for 1 month. His past medical history was unremarkable. Physical examination revealed a chronically ill appearance with neck vein distension. Heart sounds were distant but there was no murmur or S3 gallop on auscultation. The electrocardiogram showed normal sinus rhythm with right bundle-branch block. Chest x-ray revealed marked cardiomegaly. Transthoracic echocardiography revealed a large echogenic mass in the right atrium with a large pericardial effusion (Fig. 1A). Transesophageal echocardiography showed an approximately 638 cm round mass with an irregular surface, which originated from the posterior side of the left atrium and extended to the right atrium through the interatrial septum (Fig. 1B). Magnetic resonance imaging of the chest showed that the contrast-enhanced tumor occupied both atria but was mostly in the left atrium (Fig. 2). There were no signs of pulmonary vein or vena caval flow obstruction. Coronary arteriography showed a hypervascular tumor located in the atrial septum and tumor-feeding vessels originating from both coronary arteries. Surgical removal of the tumor, including the posterior wall of the left atrium, was performed. Patch repair of the interatrial septum and reconstruction of the left atrial wall with a pericardial patch were also done. On gross examination the tumor was well-defined and rubbery with a roughly dumbell shape centering on the interatrial septum. The cut surface was reddish gray and relatively homogenous, with focal fibrosis (Fig. 3A). Microscopic examination showed the typical findings of cardiac hemangioma (Fig. 3B). The patient was uneventfully discharged several days later and followed for 18 months without echocardiographic recurrence of tumor.
Reference
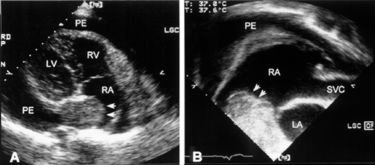
Fig. 1 (A) Transthoracic echocardiography in a modified 4-chamber view showed a large round echogenic mass in both atria across the interatrial septum. There was a large pericardial effusion. (B) Transesophageal echocardiography revealed an echogenic mass that originated from the left atrium and extended to the right atrium through the interatrial septum. LA = left atrium, LV = left ventricle, PE = pericardial effusion, RA = right atrium, RV = right ventricle, SVC = superior vena cava.
Fig. 2 Magnetic resonance T1W imaging (after contrast) shows contrast-enhanced tumor (arrow) located in the left atrium and extending to the right atrium through the interatrial septum. Abbreviations as in Fig. 1.
Fig. 3 Cardiac hemagioma. (A) The cut surface of the tumor was reddish gray, relatively homogenous, hemorrhagic, and focally fibrotic. (B) Microscopically, there are dilated cavernous vessels and small capillary channels.
Address for reprints:
Jong-Won Ha, M.D., Ph.D.
Cardiology Division, Cardiovascular Center
Yonsei University College of Medicine
C.P.O Box 8044
Seoul, Korea
Received: February 2, 1999
Accepted with revision: April 19, 1999